Everything You Need To Know About EHV-1
Learn about this highly contagious equine virus and how to curb its spread
By Christa Lesté-Lasserre, MA
Editor's Note: Reviewed and updated Nov. 24, 2025
It happens every year. First, it’s a 2-year-old that’s feverish and coughing. Then, a pregnant mare loses her foal. A week later, a seasoned sport horse becomes incontinent, falls down, and never gets back on his feet. Suddenly, you have a barn full of horses with fevers—and it seems like as soon as one gets better, two others get worse. If you’re lucky, none of the animals have moved to other locations recently where they might infect other horses.
What’s going on? Quite simply, an infectious microbe has declared war. Equine herpesvirus type 1 (EHV-1), also known as equid alphaherpesvirus-1, has awakened from the depths of its hiding place in the immune or nervous tissues of one horse, replicated, and spread out of control among horses on your premises and beyond.
Fortunately, with advancing scientific knowledge, we’re learning how to curb EHV-1’s devastating—and sometimes deadly—path of destruction. In this article we’ll present you with the basics of this equine-specific virus and how we’re managing it in light of what researchers have learned through experience and laboratory studies
What Is EHV-1?
Viruses have been infecting living cells since they first evolved hundreds of millions of years ago. Over time the microscopic agents diversified into categories depending, in part, on how they multiply, a process known as replication, using the host’s cellular machinery.
To date, scientists have discovered at least 115 members of herpesviruses affecting humans and animals. In humans, herpesviruses cause “cold sores” or skin blisters, mononucleosis, shingles, Epstein-Barr disease, and certain kinds of lymphomas. Most herpesviruses known to affect horses and donkeys primarily cause respiratory disease, says Dr. Lutz Goehring, Warren Wright Sr.-Lucille Wright Markey Endowed Chair in Equine Infectious Diseases at the University of Kentucky’s Gluck Equine Research Center.
EHV-1—and, more rarely, EHV-4—can also cause abortion. EHV-1 causes neurologic disorders. EHV-3 causes genital blisters.

Arguably, the herpesvirus that causes the most concern in the equine community is EHV-1, Goehring says. Outbreaks—albeit rare—usually start when a horse returns from an event of any kind and spreads the virus within his home farm. Far less frequently the pathogen can pop up at equestrian events, causing disease within the competition barns. If not contained, the highly contagious virus infects horses, catching a ride home with them to various parts of the country or globe.
Since the virus was first discovered in 1966, scientists have found only three variants: D752, N752, and H752. In 2021 a team led by Dr. Nicola Pusterla, professor of equine medicine at the University of California, Davis, School of Veterinary Medicine, discovered all three variants are circulating in North America as well.
While EHV-1 is technically the name of the virus itself, the term equine herpesvirus myeloencephalopathy, or “EHM” is also used to describe the neurologic disease the virus causes.

Lutz Goehring, DVM, MS, PhD, Dipl. ACVIM
Goehring is the Warren Wright Sr.-Lucille Wright Markey Endowed Chair in Equine Infectious Diseases at the University of Kentucky’s Gluck Equine Research Center, in Lexington. His Lutz Goehring Research Group focuses on equine herpesvirus type 1 and its interaction with its exclusive host, the horse.

Nicola Pusterla, DVM, PhD, Dipl. ACVIM
Pusterla is professor in equine internal medicine and chief of large animal medicine services at the University of California, Davis, William R. Pritchard Veterinary Medical Teaching Hospital. He graduated from the School of Veterinary Medicine at the University of Zurich, Switzerland, in 1991 and also earned his PhD there with an emphasis on vector-borne diseases.
What Is EHM?
In a small percentage of EHV-1 infected cases, horses develop these neurologic signs. All EHV-1 variants can provoke EHM, although the N752 genotype has become the more frequent one, Pusterla says.
Scientists are still trying to understand why some horses develop EHM, says Goehring. Tall breeds—such as Thoroughbreds, Warmbloods, and Quarter Horses—appear to be more susceptible for EHM when infected, and older horses and mares seem to develop more severe signs. It is a multi-factorial process that triggers this response.
Researchers have found EHM is likely only then when the virus gets transported away from the horse’s respiratory tract and their lymph nodes, through the bloodstream, and into the spinal cord, says Goehring.
Perhaps that’s why EHM generally appears later after infection than respiratory disease does. Gisela Hussey, DVM, MS, PhD, associate professor of pathobiology and diagnostic investigation at the Michigan State University College of Veterinary Medicine, in East Lansing, has been studying the disease and discovered horses with EHM developed fever later than those with the respiratory form of EHV-1. Horses with EHM also started showing signs of disease about nine to 13 days after infection, whereas horses with respiratory disease became sick after only four days, she says.
There has been a shift over the past two decades, says Pusteria. Against earlier belief, all varieants of EHV-1 are capable of causing EHM.
Plus, the D752 variant is the one that usually causes more cases of EHM, says Goehring. Its presence in the bloodstream—known as viremia—lasts longer, compared to the other variants, he says.
Therefore, EHM might arise from a different or delayed immune response than the respiratory form. Why horses would have that different response remains to be determined.
Horses with EHM started showing signs of disease about 9 TO 13 DAYS after infection, whereas horses with respiratory disease became sick after only 4 DAYS
What Are the Clinical Signs of EHV-1?
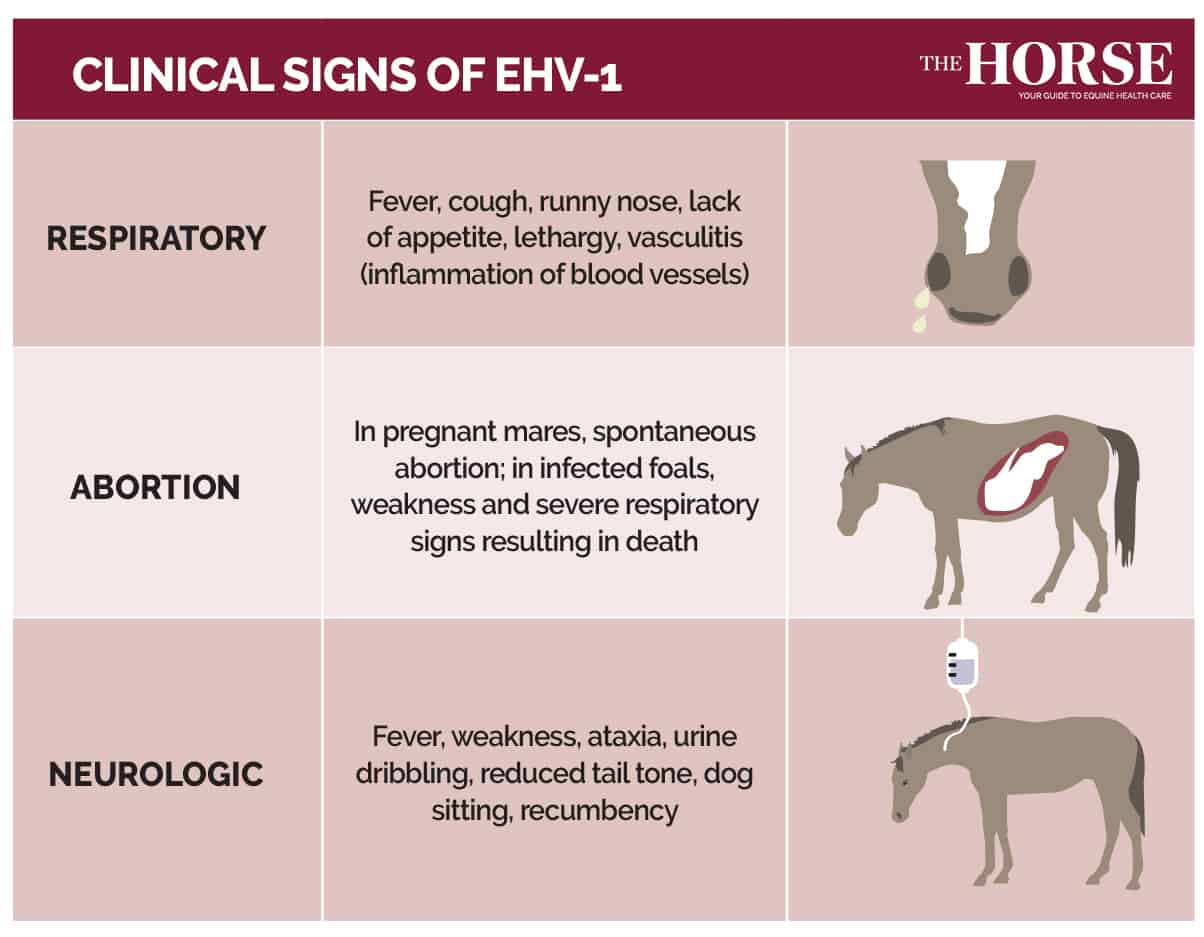
The Respiratory Form: EHV-1 can cause very subtle clinical signs that could easily go unnoticed, our sources say. Often, horses might have just a slight fever—and because they otherwise act normal and have no nasal drainage, nobody considers taking their temperature.
If they do develop obvious clinical signs, these might include a runny nose, a loss of appetite, or lethargy. Respiratory signs most commonly occur in young horses, usually younger than 4 years old. When adult horses develop a fever following the infection, it is usually due to viremia.
Some horses—especially Warmbloods and draft breeds—might develop swelling in all four limbs, Goehring says. “Very often this type of vasculitis goes along with viremia (and fever),” he explains.
The Abortion Form: Pregnant mares might spontaneously abort two to three weeks (sometimes longer) after EHV-1 infection, our sources say. Abortion generally occurs during the last three months of pregnancy. The aborted fetus and the fetal membranes (placenta) are highly infectious for other in-contact horses; so are sometimes foals that are born infected. While they succumb to severe respiratory disease, their respiratory tract fluids are highly infectious to any horses nearby, causing spread of the disease.
The Neurologic Form: Signs of EHM can appear following a fever, usually on the last day of fever associated with viremia, explains Goehring. From there, it quickly evolves into an attack on the nervous system. Horses can become so weak or ataxic (incoordinated) that they drag their hind limbs or can’t coordinate their leg movements.
In addition, horses might retain feces, dribble urine, or both, says Pusterla. Many have reduced tail tone. In severe cases horses sit down like dogs or lie down and can’t get back up again—known as recumbency.
Diagnosing and Testing for EHV-1
The current gold standard for EHV-1 testing is for veterinarians to use a swab to take a sample from the nasal tract, says Pusterla. They then send the swab to a laboratory for quantitative polymerase chain reaction (qPCR) testing.
These tests detect the presence of even small amounts of viral DNA, Goehring says. And while they don’t distinguish between dead and live viruses, they give a very good indication of whether the horse is shedding and contaminating the environment. That makes the test fast, easy, and reliable, he says.
Even so, the reliability depends on what the test is looking for, Pusterla adds. Most laboratories are currently using tests that check for either the D752 variant, the N752 variant, or both. But they’re not checking for new variants—like H752—that might be popping up. For this reason, truly accurate testing requires using a test that targets a universal EHV-1 gene. False negative EHV-1 tests that missed the H752 variant might be responsible for undiagnosed EHV-1 outbreaks in the U.S. and abroad, he says.
Laboratories must also be careful about overclassifying the results as being either an “abortion strain” or a “neurologic strain,” because all three known variants can cause both forms of the disease, Goehring warns. “Many labs started reporting the N-variant as the nonneuropathogenic variant, and that has been a mistake,” he says.
Swabbing the horse’s muzzle picks up about
Researchers have recently developed stable-side or point-of-care PCR tests that can detect EHV-1 and several other respiratory tract pathogens in horses in a single run, using a catch-all or multi-plex panel—tests that work like home COVID-19 kits, says Goehring. Such rapid testing could help prevent and manage outbreaks efficiently, but the tests are currently undergoing the final stages of validation in laboratory settings.
Because repetitive deep-nose swabbing can be uncomfortable for horses, Pusterla’s team has investigated possibilities for less invasive testing. Results from their recent study revealed swabbing the horse’s muzzle effectively picks up about 77% of the EHV-1 cases that deep nasal swabbing would have detected. This offers a promising alternative, he says, even if suspicious negatives might need to be confirmed through conventional deep-nose swabbing.
How To Treat Horses With EHV-1
Equine herpesvirus type 1 has no cure. In fact, the virus can never be eliminated from a horse’s body entirely. It stays nestled in lymphocytes (white blood cells responsible for mounting immune responses) and/or the nervous system for the horse’s life, usually in a dormant form, Goehring says.
However, during acute infection horses can benefit from supportive care and antiviral therapy, says Pusterla. Valacyclovir appears to have a strong effect against the circulation of the virus in the bloodstream, with viremia rates usually dropping to zero within a week, he says.
“It is important to control the inflammatory mediators that also cause a fever with (non-steroidal) anti-inflammatory drugs,” Goehring adds. He says he believes drugs like flunixin meglumine or firocoxib can interfere with cell-to-cell spread from viremic immune cells to the blood vessels.
Flunixin meglumine (Banamine) can help control fever, and sodium heparin can treat thromboembolism from vasculitis, says Pusterla.
“However, it is important to start as soon as possible, following the infection, with these drugs,” Goehring says, almost as in a post-exposure treatment course.
Horses with EHM can also be supported mechanically with slings to keep them on their feet, they say, but it is a tricky process and needs to be supervised by experienced individuals.
New treatments for EHV-1-related abortion are on the horizon.
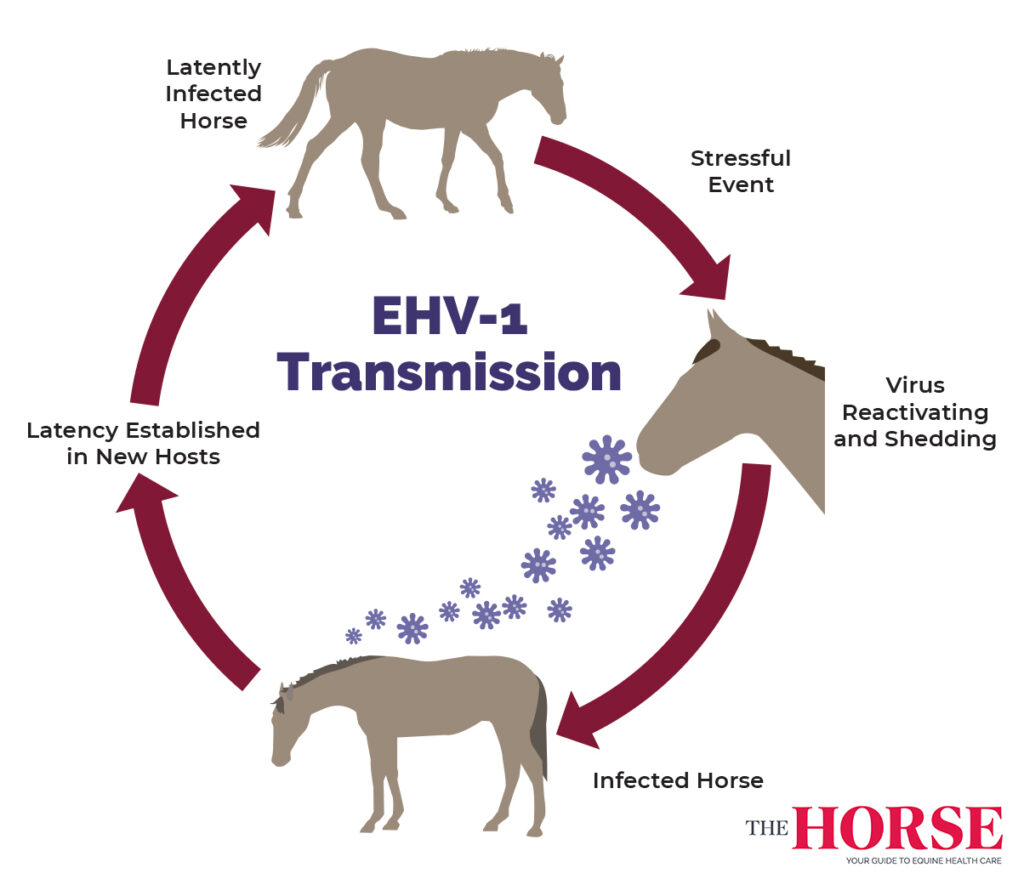
How Does EHV-1 Spread?
Most horses have acquired the EHV-1 virus by the time they reach adulthood, our sources say. And again, the virus can lie dormant in the lymphatic or neural tissues, remaining inactive for years. Outbreaks begin when dormant virus for whatever reason reactivates from latency in a single horse,. The virus returns to the respiratory tract, replicates again, and is shed into the horse’s immediate environment. While Goehring says he considers this “low-grade” shedding at best, he notes that close contact—two noses touching—and a horse with a weakened defense system create the perfect storm for production and shedding millions of virus particles through respiratory secretions. Even massive production of virus in an adult horse does not cause clinical signs such as fever or nasal discharge more than a trickle when shedding begins, allowing the virus to spread rapidly to other horses before anyone becomes aware of it. Horses nearby inhale the particles, which also land on bedding, people, equipment, and walls, where they can survive as what’s known as fomites for several hours to a few days.
Some horses are more significant shedders than others, says Goehring. Recent outbreaks have shown the existence of what he calls “Typhoid Marys”—individuals that, for whatever reason, shed much more virus than others do.
This can mean rapid viral spread to large numbers of horses, especially at competition venues where hundreds of horses are stalled in close proximity, often in indoor barns with stagnant air, and multiple horses use the same stalls and aisles over the course of several weeks, he says.
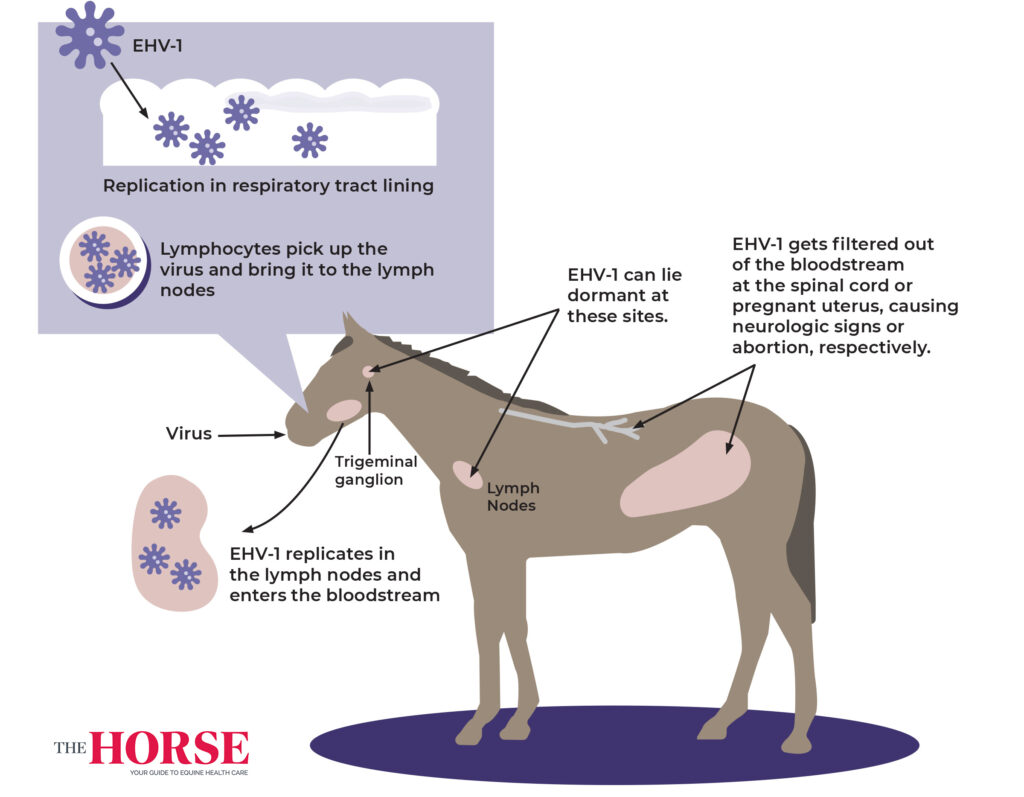
Once a horse inhales the virus, it attaches to the respiratory tract lining, where it replicates in the epithelial cells, producing “huge amounts” of virus, says Goehring. The virus gets expelled by the millions through the nostrils and also destroys cells within the horse’s respiratory tract, causing swelling, discomfort, rare coughing, and possibly secondary bacterial infections.
Meanwhile, immune cells pick up the virus as they circulate routinely through the respiratory tract and bring it into the lymph nodes. There the virus starts replicating again, this time in the lymphoid tissue. At that point it might enter the bloodstream, triggering viremia.
The bloodstream filters out EHV-1 at one of two primary sites of very specific small blood vessels: in the endometrium of the pregnant uterus or in the spinal cord. At both sites the virus causes an inflammatory response within those small blood vessels, provoking tissue destruction and sometimes even bleeding. The result is either abortion or the classic neurologic signs of EHM.
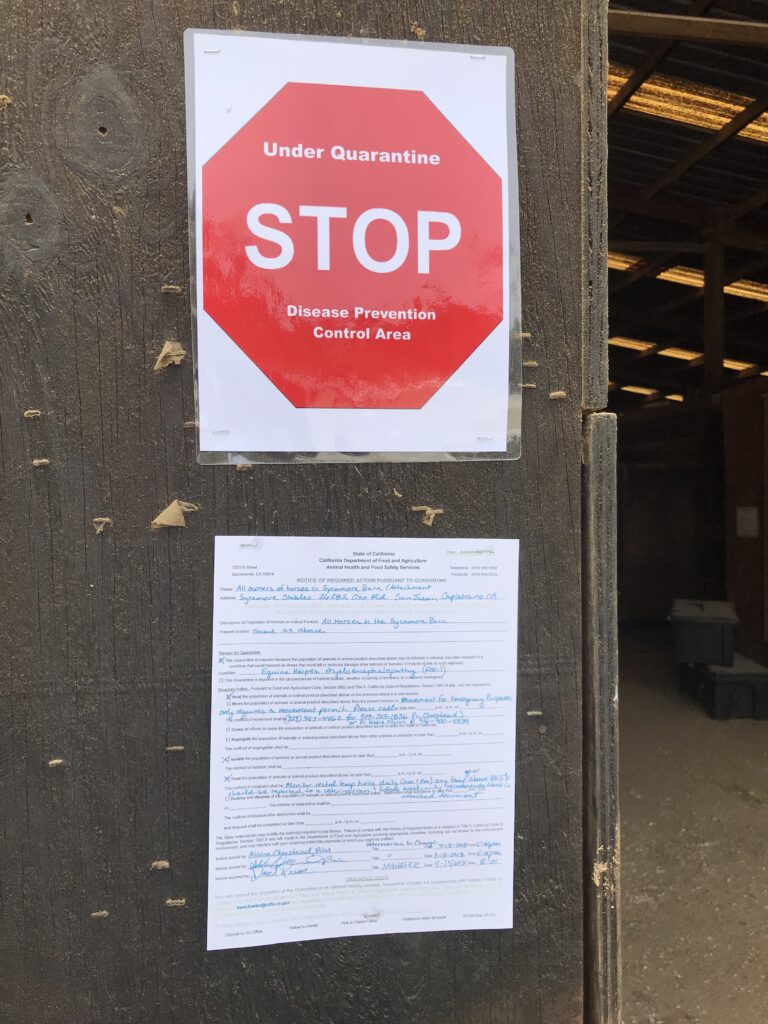
Reporting Disease Outbreaks
Equine herpesvirus outbreaks are better controlled when information is shared about their spread, which is why many states and countries have declared EHV-1 a notifiable disease, says Goehring. However, some regions dictate reporting requirements based on whether the outbreak involved EHM cases. For example, a 2016 survey in the U.S. revealed EHM to be reportable in 49 states, whereas the respiratory form of EHV-1 was only reportable in 26 states.
An added benefit of obligatory reporting is the power given to government authorities to oversee management by, for example, locking down horse movement (transport), he adds.
When it’s not obligatory, owners and veterinarians can contribute to better outbreak management through voluntary reporting. In the U.S. veterinarians are encouraged to report to the Equine Disease Communication Center, Goehring says. In Europe and elsewhere, they can contact the International Collating Centre, in Cambridge, UK.
Pathogenesis of EHV-1 in the Horse
Scientists have made great progress in understanding the pathological pathways of EHV-1 and how it spreads among horses, Goehring says. But one major mystery remains: What makes the long-low-lying virus suddenly wake up and start replicating?
EHV-1 can linger in a state of “hibernation” or latency, so to speak, in the lymph nodes or the trigeminal ganglion—the sensory part of facial nerves near the brain—leading to “a very quiet phase of viral presence,” Goehring says.
He likens this state to a veritable espionage sleeper cell waiting for the next assignment. “You can import that time bomb onto your premises,” he says. “And that’s the very dangerous and tricky part, because we don’t clearly understand what triggers this reactivation of the virus.”
A leading theory is stress or excitement reactivates EHV-1, he says. In particular, it might be related to travel stress, as many outbreaks have started after horses either return home or pass through a farm.
“We always thought that reactivation is a very rare occurrence,” Goehring says. “There is new evidence when sampling the environment at shows, at racetracks, or gatherings of horses from different places we find virus in low numbers.”
How To Prevent EHV-1
Arguably, there is no way to completely prevent EHV-1 (re)infection. Through vaccination, which increases horses’ immunity, resulting in less shedding and reduced viremia, we can lower risk of developing EHM, says Goehring.
Indeed, vaccination forms an important part of prevention. “The other important part is how much of an infectious dose reaches the horse,” he adds. “This is where other measures like distance, barriers, and biosecurity become extremely important to cut through transmission routes.”
But while vaccination helps horses fight the disease better and experience milder clinical signs, it won’t stop disease altogether, he adds. It also can’t prevent EHM.
This might be, in part, because of the vaccine’s age, as well as the “sneakiness of the virus,” he says. Veterinarians are still inoculating horses with the same EHV-1 vaccine that was developed 40 years ago.
Overhauling the EHV-1 vaccine, however, isn’t easy. The virus not only affects multiple body systems but also modulates the immune system itself, thereby evading immunity. Plus, EHM is relatively rare and, therefore, difficult to study. Most vaccine research is carried out in young horses that have never been exposed to the virus, which doesn’t reflect real-world scenarios.
Even so, several groups are working on new vaccine candidates, says Goehring. “There’s this energy to produce something more,” he says. In fact, efforts are currently underway to develop, test, and launch new RNA vaccines designed to protect horses from EHM.

Meanwhile, owners should aim to “achieve the highest possible herd immunity,” Goehring says. “It’s always better if everyone’s vaccinated, compared to only a certain percentage.”
In addition to vaccination, owners can isolate incoming horses for at least 21 days and keep show horses away from other horses and their equipment/spaces during events, says Pusterla. That doesn’t mean just sheltering horses from animals that look sick, he adds, because many actively shedding horses appear perfectly normal.
Importantly, taking horses’ rectal temperatures once or twice a day can red-flag outbreaks early and allow for rapid veterinary intervention and good biosecurity, he explains. Embedding microchips containing thermometers that automatically alert owners about temperature spikes might be critical tools going forward, he adds.
“Everybody wants to look for the magic bullet—this or that test,” he says. “But taking rectal temperature is still a very powerful tool.”
Keeping Shows Safe
Equine herpesvirus outbreaks at competitive events have led to dozens of horse deaths and hundreds of additional animals exposed to the virus, many of which have fallen ill with disease. These statistics include horses that had never been to showgrounds, because the virus travels back to home farms with horses returning from shows or any other type of event. Such outbreaks have led to multiple event cancellations and stringent movement restrictions affecting the entire horse industry in affected regions.
Governing bodies that oversee competitions have responded by ramping up biosecurity and prevention requirements at shows, says Pusterla. “The industry is realizing that EHM outbreaks are very bad for business and horse well-being,” he says. “They’ve gone from doing nothing to various biosecurity protocols, intake (or admission) exams, daily monitoring, separating/isolating sick horses, point-of-care testing of sick horses at shows, and more.”
The United States Equestrian Federation (USEF), for example, now requires competition organizers to plan for quarantine stabling, onsite treatment and supplies, and biosecurity protocols. Horses entering USEF venues must have proof of EHV-1 vaccination within the previous six months.
In 2022 the Fédération Equestre Internationale (FEI) moved to implement stringent measures to prevent sick horses from entering FEI venues, detect and isolate suspected cases rapidly, prevent viral spread, and ensure veterinary care of sick horses. Such measures include regular temperature checks—especially before entering the venue—improved stable designs for better social distancing, and rapid PCR tests (once they’ve been scientifically validated).
Both federations require negative PCR tests within specific windows of time to enter a competition following any EHV-1 outbreak in the region.
“It’s the combined elements of strong preventive biosecurity measures and the early detection and isolation of horses that are at risk of shedding (that matter in risk reduction), and vaccination may add limited protection by reducing viral shedding,” says Goran Akerstrom, DVM, FEI veterinary director.
Isolate incoming horses for at least
21 DAYS
Biosecurity Recommendations
Because EHV-1 is such a “tough to diagnose”—thus silent disease—at the beginning,” biosecurity is critical, says Goehring. During an active outbreak, property owners should establish a rapid, rigid quarantine of the premises and isolate all shedding and/or febrile horses from other horses.
EHV-1’s main route of transmission is horse to horse—and especially nose to nose direct touching, Goehring says. So owners should keep horses from all physical contact with each other during an outbreak, including the ones that had negative nasal swabs the day before, as they might be in early phases of infection. “Shedding horses should be in a separate building from the—hopefully—uninfected population,” he says.
Physical distance between horses is important, mainly because of the EHV-1’s physical characteristics, he adds. “This is not an influenza virus,” he says. “It’s not one that carries from one corner of the barn to the other within seconds or minutes. EHV-1 is a slower, heavier virus, and it travels in droplets. So, distance definitely is our friend.”
SMART BIOSECURITY STEPS
Don’t share water sources at events or during outbreaks.
Avoid nose-to-nose contact.
Isolate incoming and sick horses.

Wear protective gear, disinfect boots, and wash hands after handling sick horses.
Designate equipment for use on sick horses only.

Post-outbreak, disinfect surfaces and equipment.
EHV-1 is less likely to be transmitted via people and their clothes than it is horse to horse, Goehring says. But it certainly can travel on humans and items, so using separate equipment for sick vs. healthy horses is important, as is changing clothes and washing hands after handling each group.
“For those who like to comply with biosecurity, that involves the phone that you pick up; that involves a stethoscope, your ultrasound machine, grooming equipment,” Pusterla explains. “And it’s on the person that’s in that room. It’s on the gloves; it’s on the lab coat; it’s on the boots. It even goes as far as to the (humans’) nostrils.”
EHV-1 can remain infectious in water, our sources say, so horses shouldn’t share water sources or buckets at events or during an outbreak.
Critically, owners should never panic and try to get their horses out of quarantined premises, Goehring says. This is likely to let the virus get out along with the horse, spreading EHV-1 wherever that horse goes, with potentially disastrous consequences.
Take-Home Message
Unchecked, EHV-1 can swoop through equestrian communities, causing financial and emotional losses and compromising equine welfare. But by staying up to date on scientific knowledge about the virus and the diseases it causes, and following recommended biosecurity protocols for both preventing EHV-1 and stopping its spread, owners and veterinarians can collaborate to keep transmission—and its consequences—to a minimum.
As with COVID-19, testing for EHV-1 during outbreaks remains an enormous help to slow down or interrupt outbreak dynamics. It is money well spent, says Goehring, and should be invested in preferentially over ill-defined and untested “miracle” treatments.
Credits:

Christa Lesté-Lasserre, MA
Passionate about horses and science from the time she was riding her first Shetland Pony in Texas, Christa Lesté-Lasserre writes about scientific research that contributes to a better understanding of all equids. After undergrad studies in science, journalism, and literature, she received a master’s degree in creative writing. Now based in France, she aims to present the most fascinating aspect of equine science: the story it creates. Follow Lesté-Lasserre on Twitter @christalestelas.
Editorial Director: Stephanie L. Church
Managing Editor: Stephanie J. Ruff
Digital Editor: Haylie Kerstetter
Art Director: Claudia Summers
Web Producer: Jennifer Whittle